
ℹ️ Introduction
This article explains how to use the Ardens Manager Frailty & End of Life dashboards to understand prevalence, stratify risk, monitor activity and evaluate the quality of care across key patient groups. By the end of this guide, you will be able to use these insights to support proactive care planning, service coordination and quality improvement across your practice, PCN or ICB.
Background
Frailty and end of life care require proactive identification, coordinated management and regular review to ensure patients receive appropriate, person‑centred care. This includes those living with frailty, dementia, in care homes, or those approaching end of life.
For GP practices, PCNs and ICBs, it is important to:
Identify patients with frailty and escalating care needs.
Maintain accurate registers for vulnerable populations.
Support proactive care planning and regular review.
Monitor activity and workforce involvement.
Ensure consistent, equitable access to care and support.
The Ardens Manager Frailty & End of Life dashboards provide population‑level oversight across multiple related services, supporting integrated, proactive care delivery.
How Ardens Can Help
The Ardens Manager Frailty & End of Life suite brings together dashboards for:
Frailty
End of Life
Dementia
Care Home
Housebound
Deaths
Across these services, users will find a combination of:
Registers and population insights
Risk stratification (where applicable)
Activity monitoring
Safety alerts
Case finders
Performance indicators
Each dashboard follows a consistent structure, allowing organisations to manage vulnerable patient groups using a single, unified approach.
The dashboards work alongside existing Ardens Clinical resources to support proactive care planning and coordinated delivery. To learn more about the clinical resources, access the support articles below:
✅Included in Ardens Manager National Content package: Interested in finding out more or requesting a trial? Contact accounts@ardens.org.uk
📍 Access the Dashboard
Log into Ardens Manager.
Go to Services on the left-hand pane.
Open to Conditions folder.
Click on Frailty & End-of-Life.
Click on the required condition tab.
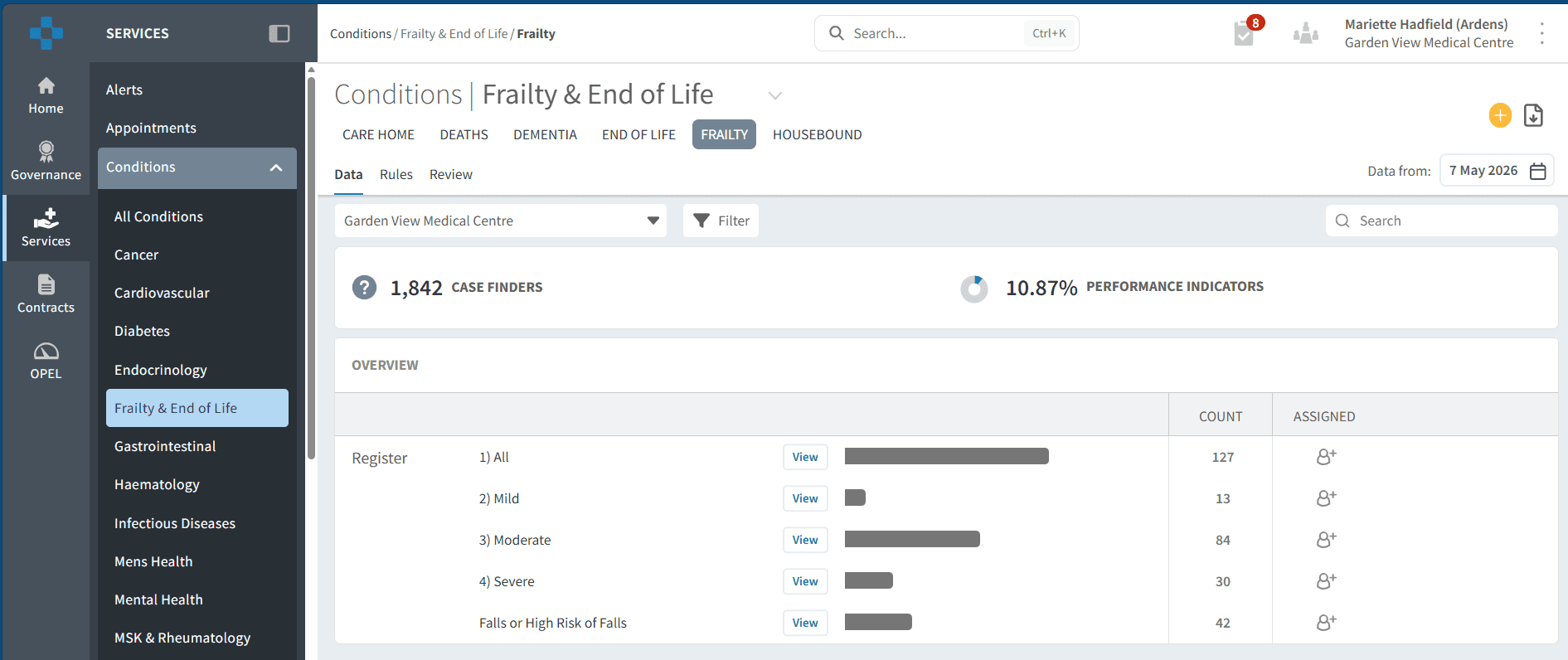
📊 Plan & Forecast Demand
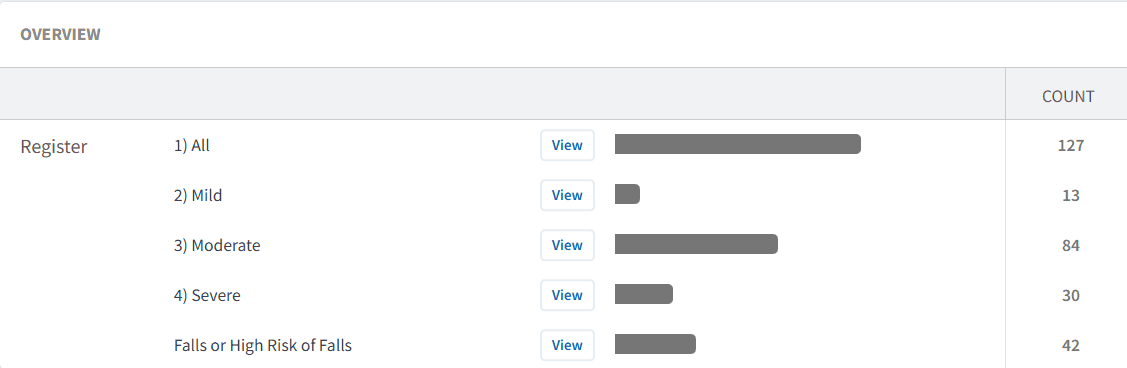
The Overview sections support identification of vulnerable populations and planning of proactive care.
Understand Your Population
Registers provide visibility of patients across frailty and end of life pathways, including:
Frailty cohorts
Patients on end of life registers
Care home residents
Patients with dementia
Housebound populations
These reports help organisations understand:
Recorded prevalence.
Population characteristics.
Coding patterns and register accuracy.
Size of the cohort requiring proactive review and support.
Levels of clinical complexity and need (where available).
This insight supports informed workforce planning and recall scheduling.
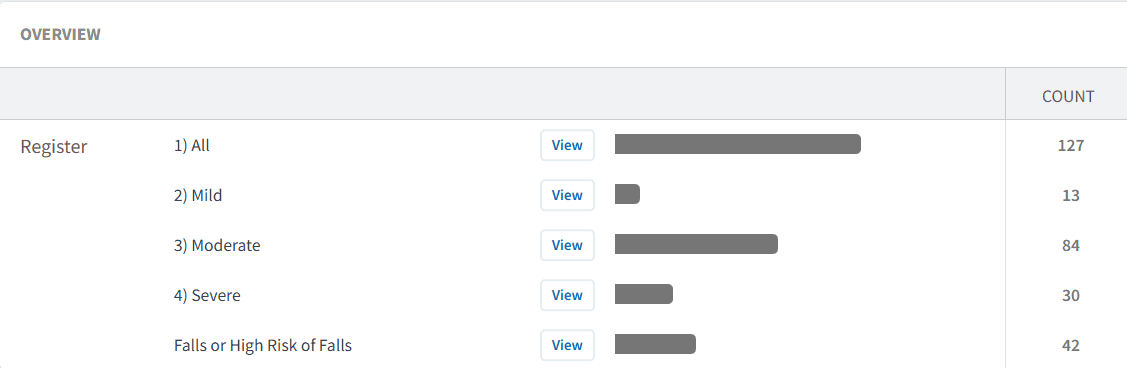
To review registers:
Click the View button next to the required register report.
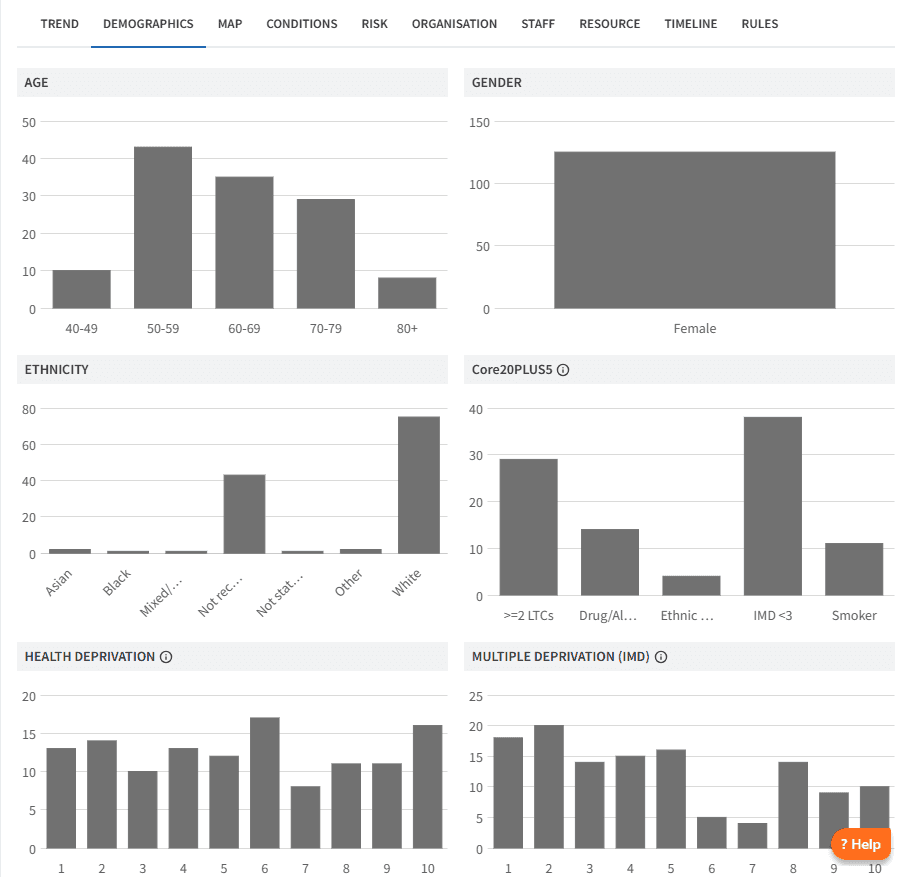
Review the Demographic tab to understand age distribution and deprivation.
Review the Conditions tab for breakdown by long-term condition and multimorbidity.
Review the Risk tab to identify patients in vulnerable or higher-risk groups.
Further insights allow organisations to review diagnosis patterns by clinician and by patient geography, supporting identification of variation and unmet need.
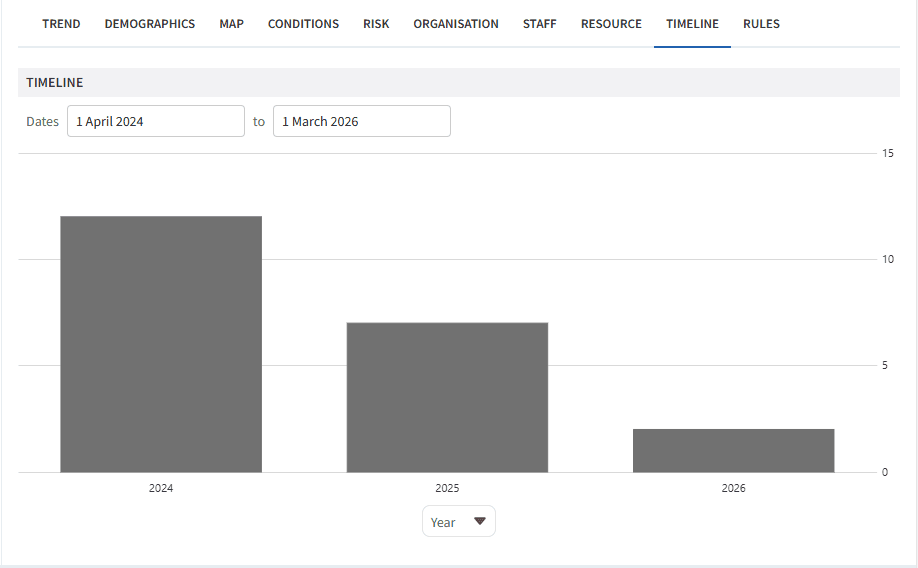
Analyse Trends
Understanding how registers change over time allows organisations to anticipate workload and monitor the impact of case-finding and prevention activity.
To analyse trends:
Click View next to the required report.
Click on the Timeline tab.
Choose Year (or another timeframe) from the drop down below the chart
This allows you to:
Analyse trends in diagnosis rates.
Identify an increase in demand.
Inform capacity considerations vs potential demand.
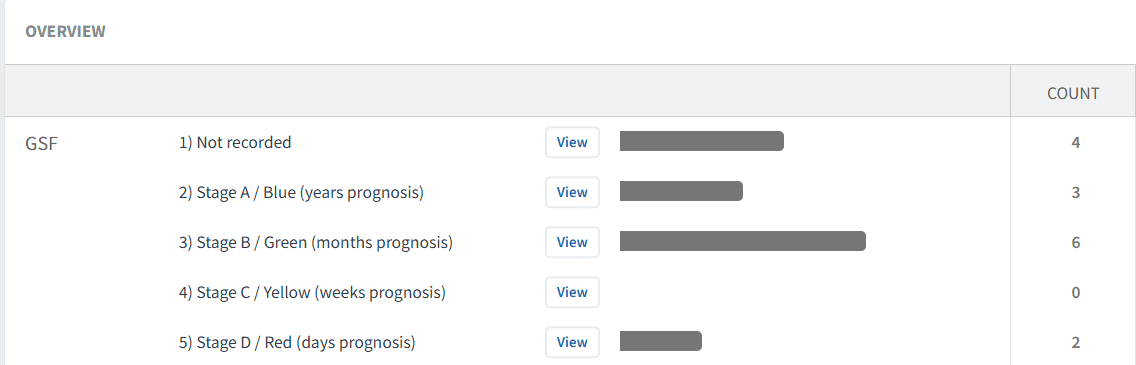
Condition Specific Risk Stratification
Some dashboards within the suite include risk stratification to support prioritisation such as Gold Standards Framework (GSF).
This enables organisations to:
Identify patients approaching end of life.
Monitor distribution across GSF stages.
Support proactive care planning and multidisciplinary review.
Using this insight, teams can prioritise:
Advance care planning.
Regular review and follow‑up.
Coordinated, person‑centred care delivery.
🔎 Monitor Activity & Safety
The dashboards provide tools to support clinical governance, patient safety and service oversight.
Last Month Activity
All diabetes dashboards include a summary of activity for the previous month, including:
New diagnoses.
Reviews and monitoring completed.
Workforce involvement by role.
To review activity:
Click View next to the activity report.
Review the Demographic, Conditions, Risk and Staff tabs.
Analyse the Timeline tab to understand recent trends.
Safety Alerts
Safety Alerts highlight patients who may require urgent review or follow-up, such as:
Missing care plans or reviews.
Indicators of increased vulnerability or deterioration.
Potential gaps in monitoring or coordination.
For each report:
Click View.
Select PATIENTS tab.
Review each patient and take appropriate action.
This supports monitoring of workload, capacity and delivery against local priorities.
Case Finders
Case Finder reports support identification of:
Patients who may meet criteria for inclusion in frailty or end of life registers.
Patients with missing or incomplete coding.
Individuals requiring review or reassessment.
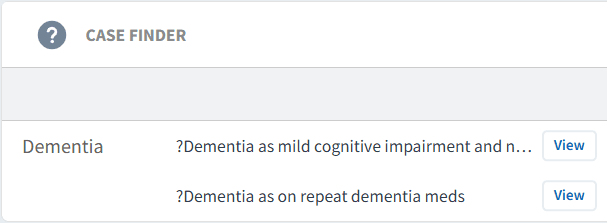
Using case finders:
Click View.
Select PATIENTS tab.
Review each patient record.
If diagnosis is confirmed:
Add the appropriate diagnosis code in the clinical system.
This will move the patient onto the register and remove them from the case finder.
If inclusion is due to a data error:
Amend or remove the incorrect coding in the clinical system.
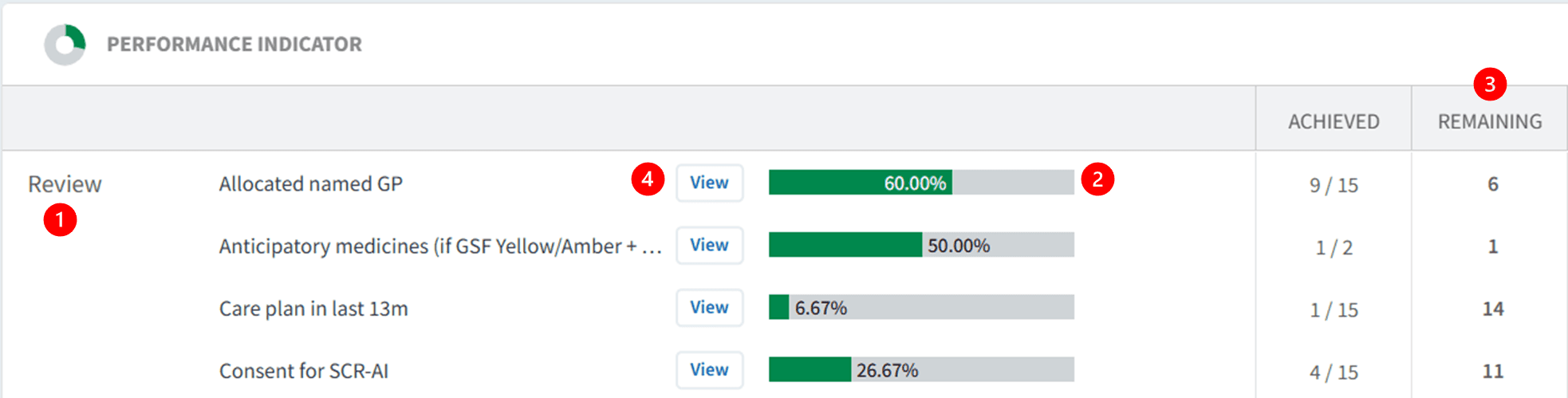
Performance Indicators
Performance Indicators support monitoring of key care components, such as:
Completion of care planning.
Review activity.
Documentation of key elements (e.g. advanced care planning, dementia reviews).
Reviewing performance indicators:
Indicators are grouped by diagnosis, review, target or screening.
Green bars display percentage completion.
The Remaining column highlights outstanding care.
Click View and select Show remaining only to support follow‑up.
⚠️ Please note: Patient data can be exported. Refer to this support article for further information.
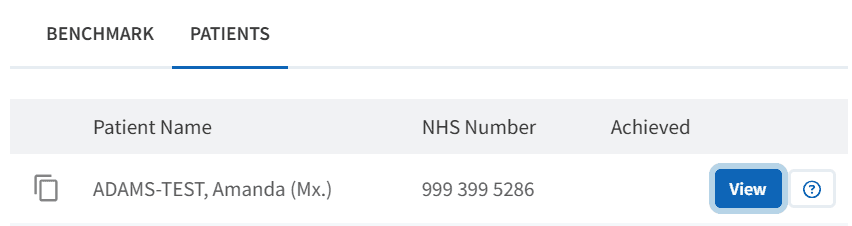
Patient View for Follow-up
The Patient View functionality enables clinicians and teams to review outstanding elements of care at an individual patient level.
To access Patient View:
Click View next to the patient’s NHS number
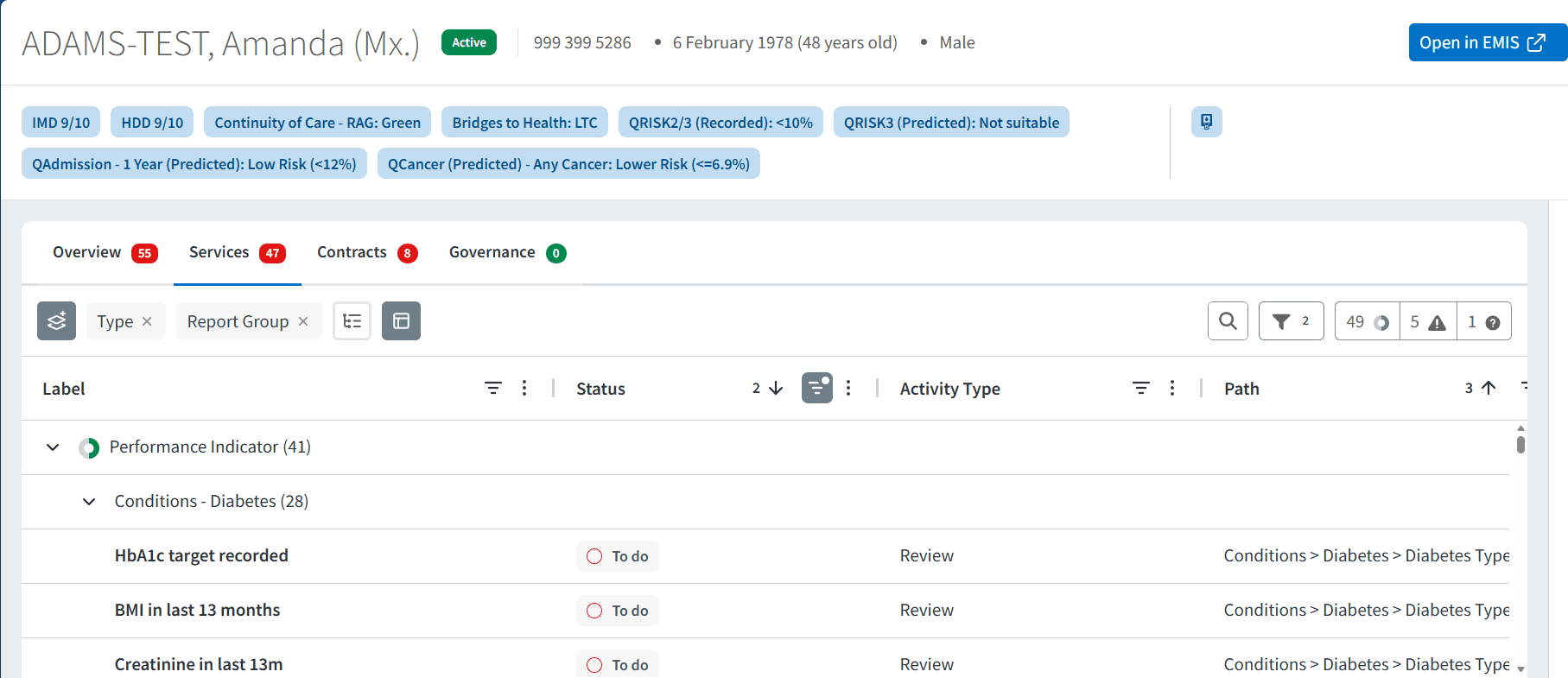
Within the patient view:
View all Ardens Manager findings for the patient across relevant reports
Highlight what still needs action
Use this as a prompt list, then review clinical details (history, repeat/long-term use, appropriateness) in the clinical system record
To take action:
Click Open in EMIS/SystmOne to review the full clinical record
Assess suitability of alternatives
Consider patient preference and clinical need
Complete any required medication changes
❓FAQs
What time period does 'Last month activity' refer to?
This reflects activity recorded in the previous calendar month and is updated regularly as data refreshes.
How do case finder reports work?
Case finders identify patients who may meet criteria for diabetes or pre-diabetes but are not coded. These should be clinically reviewed and coded appropriately if confirmed.
How do the dashboards support proactive care?
By highlighting high-risk patients, unmet care needs, and trends, they enable targeted interventions rather than reactive care.
🏫 Additional Support
To further your understanding of the Ardens Manager platform:
Book training for your GP Practice, PCN or ICB.
Contact our Support Team for support in real time.